
The Church Of The Bystanders —> Article
The Mass Shooting and Liberal Utopian Society
Written by: Pastor Andrew Isker
In the last two weeks, there have been two mass shootings in the United States, and the second took place this week at an elementary school in Uvalde, Texas. These shootings have reignited the regime’s already intense desire for a disarmed populace. Even before the bodies of the dead children had been removed from the school, our mentally diminished President spoke to the nation, demanding that rifles (which he is not even able to accurately describe) be confiscated across a 330 million person country spanning an entire continent.
This despicable man, and the legion of sociopathic ghouls arrayed behind him, are clearly overjoyed that there is a classroom full of young children lying dead in Texas. They don’t actually care about the anguish of parents who will never see their child grow up. Their deaths are merely a political prop for the most evil people on the planet.
It is hard to fully comprehend just how totalitarian such designs are. But these are the very same sadistic freaks who successfully locked those 330 million people in their homes for weeks or months, and then (mostly successfully) restricted their ability to provide for their families if they refused to get an extremely dangerous mRNA injection that does not even accomplish its intended purpose. All you are to them is a guinea pig or a rat in a social experiment. You do not matter. Your children do not matter. You only exist to provide them with power.
You must understand that school shooters and other mass shooters are an extremely acute symptom of the disease that horribly afflicts the American nation. You live in an incredibly sick society, and since you are born into it and live in it every day, you go about your life mostly unaware of just how dreadful things really are. It is imperative for the people who manufacture the inversion of reality that you perceive everything through the lens of the now.
This is why “The Current Thing” has such memetic power: it attacks reality distortion at its source, where obsession over what is, right now, cuts you off from any sense of historical perspective. In the case of mass shootings, the exclusion of historical perspective keeps the masses from noticing that mass shootings are a very recent phenomenon and that decades ago, when the United States had vastly more liberal gun laws, and anyone could even purchase fully automatic submachine guns in the mail, this never happened. The question you should ask is, why not? What exactly was different about America 90 years ago compared to today?
The answer to that question is fairly obvious. Modern American society is a factory for psychopaths. The young man in the North American Continent is planted in a field fertilized by atomization, loneliness, and hopelessness. Many have never met their father, and most do not have anything remotely close to a “good relationship” with him. Most have no meaningful connection to the community in which they live, nor even the nation they inhabit. In school, they are social outcasts, driven to niche internet communities for the only semblance of human interaction in their lives. They are marinated in hardcore pornography from before they have even reached pubescence.
They know (or at least perceive) that they will never know the love of a flesh-and-blood woman. They are on the kind of pharmacological cocktail that any premodern society would only ascribe to witchcraft and demon possession. They have nothing to live for and no one who loves them. Given how many young men our nation is producing like this, the question we ought to be asking is not “why does this happen?” but rather “why does it not happen a lot more?”
America is an incredibly sick nation. There is a spiritual sickness that pervades everything like a dark cloud. The people who dominate every institution in our nation have held this power for at least sixty years. For these sixty years, they have treated this nation as a grand social experiment. They have made the natural family, the very bedrock of human civilization, an antiquated, outdated institution that we have progressed beyond.
They have financialized and commodified all of human life, uprooting people from their homes and extended families, and making them mercenaries chasing after a rapidly devalued dollar. They have exported the industry of the nation impoverishing the heartland of the country and leaving them to languish in despair. They actively cheer the deaths and replacement of the hated population, while at the same time denying this was ever their intent. They have introduced racial and ethnic strife, and in the chaos actively undermined rule of law. Sixty years of full-spectrum control by utopian social engineers have transformed the most affluent society in human history into hell on earth.
This did not happen by accident. These people are motivated by a deep hatred of humanity. Like the geriatric that currently occupies the Oval Office who well represents them, they simply do not care how much people suffer. You might think the progressive is merely mistaken, deluded by ideology. This is not the case. They have had more than sixty years to see the full extent of human misery their ideology produces when applied to the healthiest and most prosperous conditions. They know what they are doing.
But what is to be done? The utopian bugmen that dominate our nation must be overcome. You must personally re-capture the same spirit of Christian America that built a great nation. You must do all within your personal sphere of influence to rebuild the things that our enemies have destroyed. You must rebuild churches dominated by liberals and weak-willed conservatives. You must rebuild neighborhoods and communities with people who, like you, love the nation that their great, great-grandparents built and who want to worship the same God who gave them such strength.
You must devote your life to both retaking what institutions you can, and creating alternatives for the institutions you can’t. It is not simply enough to decry that the libs have ruined everything—of course they have, they are like cancer! You must have a vision for your people, you must provide for them the thing they have taken away: hope for the future. We can again have the world that the liberal globalist regime has destroyed. A world where the fear of the Triune God pervades the land and not hopelessness and despair. You can have a world where things like mass shootings never happen again, but you must devote yourself to a life of repentance, faith, and an unquenchable passion for the true, good, and beautiful things God has given.
About The Author
Andrew Isker is the pastor of 4th Street Evangelical Church in Waseca, MN. He is a graduate of Minnesota State University and Greyfriar’s Hall Ministerial Training School, and he has served churches in Missouri, West Virginia, and Minnesota. He is the author of the forthcoming book, The Boniface Option. Andrew, his wife Kara, and their five children reside in his hometown of Waseca, MN. He can be found on Gab @BonifaceOption.
COVID-19 Initial Update // May 3rd, 2021
Quote from a blog:
The biggest shock to me is how many people are willing to collude in the deception by deceiving themselves first.
October 26, 2021: The FDA Advisory Panel has lost it conscious. It now has recommended COVID injections for children. This is what they think of our children:
"We're never going to learn about how safe this vaccine is unless we start giving it," Dr Rubin said, urging other panelists to vote for it. "That's just the way it goes."
This callous comment , “That’s just the way it goes” reveals the moral depravity of the panel - too bad if you lose your child- Dr. Rubin is Editor for The New England Journal of Medicine- I am sure you can trust the NEJM. These are physicians who took an oath “to do no harm”. They have drank the Kool-Aid of “societal good” - just as NAZI physicians- they forget if you do away with the individual you will have no society.
http://www.informationliberation.com/?id=62628
**************************************************************************
September 17, 2021: 16/18 FDA seated panelists vote against booster shots for the healthy/children—- apparently some are getting a conscious——- THIS IS HUGE!!!! ****************APPARENTLY NOT ****************
https://tapnewswire.com/2021/09/its-complete-nonsense-killing-two-people-to-save-one-life-injuries-extra/#comment-84678
****************************************************************
YES WE DO EARLY COVID TREATMENT-CALL IF YOU NEED TREATMENT. THE EARLIER THE START OF TREATMENT THE BETTER!!
BEFORE YOU CALL GET A PULSE OXIMETER IF YOU CAN AS THIS HELPS GUIDE TREATMENT
Call 770-530-3342
EARLY TREATMENT WORKS (studies prove it): https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8088823/
For those of you who wish to research nutraceuticals:
https://p.widencdn.net/kvdwlh/COVID-19_Nutraceutical-and-Botanical-Recommendations-for-Patients_v4
******************************************************************
BEFORE YOU TAKE A COVID “VACCINE” PLEASE EDUCATE YOURSELF. THIS BLOG CAN BE YOUR STARTING POINT.
May 11,2021: https://rumble.com/vgw2x9-doctors-testify-before-texas-state-senate-to-oppose-mandatory-covid-s-plus-.html
If you cannot watch the full video at least watch minutes 43-45.
This is a long but well written article:
https://www.technocracy.news/blaylock-on-vaccines-what-you-need-to-know-for-informed-consent
PLEASE PLEASE DO NOT GIVE YOUR CHILDREN A COVID “VACCINE” !!!!!
From the World Health Organization’s own website (even they admit the “vaccine” is not a good idea for children):
“Children and adolescents tend to have milder disease compared to adults, so unless they are part of a group at higher risk of severe COVID-19, it is less urgent to vaccinate them than older people, those with chronic health conditions and health workers.
More evidence is needed on the use of the different COVID-19 vaccines in children to be able to make general recommendations on vaccinating children against COVID-19.”
https://www.who.int/emergencies/diseases/novel-coronavirus-2019/covid-19-vaccines/advice
British not vaccinating all children: https://www.telegraph.co.uk/politics/2021/07/17/children-will-get-covid-vaccines-vulnerable/
September 13, 2021:
SARS-CoV-2 mRNA Vaccination-Associated Myocarditis in Children Ages 12-17: A Stratified National Database Analysis
https://www.medrxiv.org/content/10.1101/2021.08.30.21262866v1
****************************************************************
COVID< COVID< COVID< COVID
The “scientific” discussion that follows is not meant to be complete nor completely referenced as I have a job, family, and other time demands. There will be antidotes and occasional opinions so please excuse. Do your due diligence and investigate yourself (yes it requires effort).
Any discussion of the Covid virus or Covid vaccine must be grounded in education and ethics. For one to discuss the Covid virus or vaccines certain levels of intellect and education are required. Assuming intellect is present, then education in science is a must.
Most people profess “belief “in science, rather than expend the energy and work required to obtain the “knowledge “of science. “Belief” is a feeling, not a concrete basis for a scientific discussion. Actually, voiced “belief” is often the antithesis of scientific discussion. Science strives not for “belief”, but facts of knowledge.
Quote:
Denial-ism/Confirmation bias; what prevents people from seeing the Truth when presented with facts.
“I have yet to meet in my life someone who allowed a fact to overwhelm a belief. Once you’ve adopted a belief, facts are not welcome because what they do is, they not only indict your belief, but they indict the energy that you hold that says, “I have to believe what I’m told.” Denialism/Confirmation bias; what prevents people from seeing the Truth when presented with facts.
______________________________________________________________________________________________________________________
This paragraph added June 4, 2021 in response to intelligent people unable to reconcile scientific facts(this should be in Psychology section):
People see what they wish to see. This is a psychological fact. Change a person’s emotion and that changes their perception, perception dictates their “rational” actions which may or may not coincide to reality. Pay attention here: what appears “rational” to you depends on your perception which is controlled by your emotion and your “rational” thought or action is controlled by your perception which may NOT coincide to reality.
Why is this so important ? Because there has been a several decades long attempt to get the population to “feel” rather than use logic. Emotions are easier to manipulate than logic. Example is: “ I have my truth and you have yours”. Truth is reality and cannot be two different things. Please shed your emotions and look at facts. One fact is there are BAD people.
Quote:
“Logic can be met with logic, while illogic cannot—it confuses those who think straight. The Big Lie and monotonously repeated nonsense have more emotional appeal … than logic and reason. While the [people are] still searching for a reasonable counter-argument to the first lie, the totalitarians can assault [them] with another.”
Joost Meerloo, The Rape of the Mind
FRUSTRATED PHYSICIAN :
https://www.bitchute.com/video/Ndflatx0NP9i/
______________________________________________________________________________________________________________________
I HAVE GROUPED THE DISCUSSION INTO THE FOLLOWING CATEGORIES (lot of overlap):
1) ETHICS 2) COVID Virus 3) COVID “VACCINES “ 4) Treatment 5) PSYCHOLOGY 6) THE SOLUTION
_______________________________________________________________________________________________________________________
1) ETHICS
“Ethics” should not have to be discussed in a legitimate moral society. As our society, indeed the world, has descended into the secular abyss and absolute religious moral standards have disappeared, thus requiring “ethics” to be taught. These “ethics” grounded in the shifting sands of “feelings” and societal expediency requires constant “reeducation” as new and “obsolete” ethics are at play. It would be too simple to abide by a simple moral rule of “do unto others as you would have them do unto you”.
To that end of supplying ethical rules for a destitute society I give you here a copy of the secular Nuemberger Kodex used to pass death sentences on German physicians and Nazi party members after World War II (what is good for the gander should be good for the goose). Much of this is from Wikipedia.
On August 19, 1947, the judges delivered their verdict in the "Doctors' Trial" against Karl Brandt and several others. They also delivered their opinion on medical experimentation on human beings. Several of the accused had argued that their experiments differed little from pre-war ones and that there was no law that differentiated between legal and illegal experiments.
In April of the same year, Dr. Leo Alexander had submitted to the Counsel for War Crimes six points defining legitimate medical research. The trial verdict adopted these points and added an extra four. The ten points constituted the "Nuremberg Code". Although the legal force of the document was not established and it was not incorporated directly into either the American or German law, the Nuremberg Code and the related[1] Declaration of Helsinki are the basis for the Code of Federal Regulations Title 45 Volume 46 [3], which are the regulations issued by the United States Department of Health and Human Services governing federally-funded research in the United States. In addition, the Nuremberg code has also been incorporated into the law of individual states such as California, and other countries[citation needed].
The Nuremberg code includes such principles as informed consent and absence of coercion; properly formulated scientific experimentation; and beneficence towards experiment participants.
The ten points of the Nuremberg Code
The 10 points are, (all from United States National Institutes of Health) [2]
The voluntary consent of the human subject is absolutely essential. This means that the person involved should have legal capacity to give consent; should be so situated as to be able to exercise free power of choice, without the intervention of any element of force, fraud, deceit, duress, over-reaching, or other ulterior form of constraint or coercion; and should have sufficient knowledge and comprehension of the elements of the subject matter involved as to enable him/her to make an understanding and enlightened decision. This latter element requires that before the acceptance of an affirmative decision by the experimental subject there should be made known to him the nature, duration, and purpose of the experiment; the method and means by which it is to be conducted; all inconveniences and hazards reasonable to be expected; and the effects upon his health or person which may possibly come from his participation in the experiment. The duty and responsibility for ascertaining the quality of the consent rests upon each individual who initiates, directs or engages in the experiment. It is a personal duty and responsibility which may not be delegated to another with impunity.
The experiment should be such as to yield fruitful results for the good of society, unprocurable by other methods or means of study, and not random and unnecessary in nature.
The experiment should be so designed and based on the results of animal experimentation and a knowledge of the natural history of the disease or other problem under study that the anticipated results will justify the performance of the experiment.
The experiment should be so conducted as to avoid all unnecessary physical and mental suffering and injury.
No experiment should be conducted where there is a prior reason to believe that death or disabling injury will occur; except, perhaps, in those experiments where the experimental physicians also serve as subjects.
The degree of risk to be taken should never exceed that determined by the humanitarian importance of the problem to be solved by the experiment.
Proper preparations should be made and adequate facilities provided to protect the experimental subject against even remote possibilities of injury, disability, or death.
The experiment should be conducted only by scientifically qualified persons. The highest degree of skill and care should be required through all stages of the experiment of those who conduct or engage in the experiment.
During the course of the experiment the human subject should be at liberty to bring the experiment to an end if he has reached the physical or mental state where continuation of the experiment seems to him to be impossible.
During the course of the experiment the scientist in charge must be prepared to terminate the experiment at any stage, if he has probable cause to believe, in the exercise of the good faith, superior skill and careful judgment required of him that a continuation of the experiment is likely to result in injury, disability, or death to the experimental subject.
Reprinted from Trials of War Criminals before the Nuremberg Military Tribunals under Control Council Law No. 10, Vol. 2, pp. 181–182. Washington, D.C.: U.S. Government Printing Office, 1949. Note that complete electronic copies of the Trials of War Criminals Before the Nuernberg [Nuremberg] Military Tribunals Under Control Council Law No. 10 [3] are available online, as are most of the other proceedings from the Nuremberg Trials.[4]
**************************************************
BRITISH MEDICAL JOURNAL No 7070 Volume 313: Page 1448,
7 December 1996.
CIRP Introduction
The judgment by the war crimes tribunal at Nuremberg laid down 10 standards to which physicians must conform when carrying out experiments on human subjects in a new code that is now accepted worldwide.
This judgment established a new standard of ethical medical behavior for the post World War II human rights era. Amongst other requirements, this document enunciates the requirement of voluntary informed consent of the human subject. The principle of voluntary informed consent protects the right of the individual to control his own body.
This code also recognizes that the risk must be weighed against the expected benefit, and that unnecessary pain and suffering must be avoided.
This code recognizes that doctors should avoid actions that injure human patients.
The principles established by this code for medical practice now have been extended into general codes of medical ethics.
I ask one after educating themselves in the “science” to apply the same secular “ethics” to the current situation and participants that was applied to the German physicians in 1947.
***********************************************************************************
FOR INFORMED CONSENT REGARDING “VACCINATION” THE FOLLOWING QUESTIONS NEED TO BE ANSWERED:
Following are questions that need to be asked and answered (I cannot take credit for them, rather someone on an email thread I was on asked them- whoever I copied, thank you.):
What is the data on actual absolute reduction of transmission? What is the peer reviewed data proving the ” vaccines” stop transmission?
2. What about pathogenic priming\immune enhancement - what is the absolute and relative risk data showing this cannot occur??
3. What about potential long-term immune dysfunction related to continued production of spike protein, depletion of antibody production as a result, or immune cross reactivity with placenta/sperm causing infertility and miscarriages?
4. What is the data proving that the mRNA is destroyed in a few hours?
5. What is the compensation policy for people being forced to take any of these “vaccines”, when every vaccine ever made has known complications? How does one apply for compensation if one is injured by these products?
6. What exactly are the known potential short term and long term complications of taking this injection?
7. What peer review research papers of Pfizer, Moderna and Johnson and Johnson vaccines is available to review and read? Can I be provided copies of the peer review studies?
8. Full disclosure on actual absolute statistical efficacy versus relative statistical efficacy
9. Based on well documented severe injuries from previous mandated vaccines, for example anthrax, H1N1, dengue fever vaccine, why do I not have a right to decide whether to take my chances with the disease versus the pharmaceutical products? What exactly is my risk -benefit ratio??
10. Since these products do not fit the classical previous definitions of vaccines, and are novel mRNA technology, why are we not allowed to refuse it?
11. Why are there so many chemicals in each of the vaccines? One preservative should suffice? What studies are there documenting in humans the known potential adverse effects of each of these compounds when injected systemically and what the known toxic dose of each??
12. If the “vaccine companies” claim their products provoke an immune response, but use artificial chemicals to do so, what proof is there that a normal immune response is so provoked, what cellular immunity long term studies are available? How long do the antibody titers last, and in patients recovered from actual Covid, which provides the best long term immune response - the antibody titers or the T cell immunity - and how do can that be verified and tested for??
13. In a disease that currently has a 0.4-0.6 % death rate, no more than 1.3% in the very high risk, and with recent WHO data showing that cases were overestimated due to cycles of replication over 35% or more giving over 80% false positive rates, and overall 0.001% death rate worldwide, why are governments trying to mandate these products? And there are pharmaceutical and nutraceutical combination treatments that used early (and even late in the case of ivermectin) almost always result in recovery, even in high risk patients. As part of my informed consent, why are alternatives like this not being discussed?
14. It is well known there are multiple strains of coronavirus, any of which could mutate at any time, like influenza viruses, and this phenomenon may already be occurring with these vaccinations, and the abnormal immunity produced by them may even be causing some of the mutations. In which case when will the endless vaccinations stop? Herd immunity has worked for all of the other respiratory pandemics in the past. We should be allowed and offered the choice between developing natural immunity versus a chemical concoction, like any informed consent on any procedure - what are the risks, benefits and alternatives??
15. Inform all recipients of the injections that this is currently an EUA product, and thus not approved by the FDA as yet.
16. Finally, all potential recipients should be given a list of all the additives and chemicals in each “vaccine” prior to administration so that they can report potential allergic reactions and have the data to understand exactly what is administered.
All physicians who believe in the Hippocratic oath should be able to answer these questions for their patients, all facilities offering these novel “so called vaccine “ products, should be giving the same informed consent.
Finnish Legislator:
https://rapsodia.fi/covid-vaccine-genocide-english-subtitles/
2) COVID VIRUS
Viruses in nature do not become more lethal (science fiction or man made) as the virus would also die. Viruses wish to be like the common cold- a nuisance to everyone not just a few, with no mortality otherwise they die also.
************************************************
What does the COVID virus do in the body? Acutely appears to attack the endothelial tissues of blood vessels that are ACE2 receptor rich such as brain, heart, lung and kidney. Other pathways will be discovered for the acute phase probably.
Long term effects are unknown at present. Fear would be that the viral antigens would cross react with other human tissues or cause antibody response to human tissues like strep antibodies cause rheumatic fever ( we do not treat a strep throat for the sore throat, but rather to prevent the body from making antibodies that end up attacking your heart valves.)
In depth look:
https://www.nature.com/articles/s41586-020-2286-9
********************************************
QUESTIONS:
Where did the virus come from? China.
https://www.youtube.com/watch?v=YeW5sI-R1Qg
Accident or deliberate? No “one “ (general public) knows for sure
Virus modified or natural? Unknown, but a lot of coincidences. Wuhan lab working on “Gain of Function”( called weaponization) with coronaviruses, funded by the US NIH (say Fauci). (Say Ralph Baric). See NewsWeek magazine October 2020 and below intelligencer article.
https://nymag.com/intelligencer/article/coronavirus-lab-escape-theory.html
UPDATE: 5-10-21: https://thebulletin.org/2021/05/the-origin-of-covid-did-people-or-nature-open-pandoras-box-at-wuhan/
Update: June 22, 2021- video portion:
https://www.wsj.com/articles/are-covid-vaccines-riskier-than-advertised-11624381749
July 15, 2021: For those who wish to track events of the “pandemic” and who profited :
https://brandnewtube.com/watch/dr-david-martin-dr-reiner-fuellmich-july-9-2021_RlmKScwsMf6ATEG.html
June 7, 2021: Not to be left out the Pentagon got in on the action.
!! Now even the media is having to admit COVID-19 is a “designer” virus and some of the guilty parties are being exposed- It is time to bring charges for CRIMES AGAINST HUMANITY.
Opinion: Never like to accept a “cure” from the person who was the cause.
Mortality is currently below flu, would have been even lower if early treatments had been instituted.
Death rate for persons over 70 less than 5%.
Death rate in young adults less than 0.3%
Death rates in children less than 0.01%.
Co morbidities certainly a factor in mortality- elderly, obesity, diabetes, HBP just like in all diseases.
Why use incorrect testing when a test was developed in 2005 (read the conclusion section)?
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1232869/
Kary Mullis warned repeatedly that PCR, for whose discovery he received the Nobel prize, CANNOT diagnose any pathogen.
The PCR will fluoresce when it detects something, and we detect the fluorescence. This is an oversimplified, but quick explanation: if a fluorometer is used to detect total fluorescence (not a gel, where you can match bands) the detector would not be able to distinguish which band the fluorescence is from. Note: PCR can be qualitative or quantitative, however the tests approved for emergency use are qualitative ones only. When fully matching sequences are not present any ssDNA (if you’re not aware, PCR first converts the viral and any other RNA in the sample to DNA before amplifying it) and PCR primers without matches will anneal to any other ssDNA with partial matching sequences. Only 6 nucleotides matching the sequence of any DNA at the 3’ end will initiate enzymatic primer extension. Random amplification can occur if any nontarget DNA with two segments partially matching in the mix to initiate. PCR amplification of unintended DNA is well known and has been described in numerous scientific journals.
MAYBE THIS IS WHY THE “FLU” DISAPPEARED LAST YEAR:
After December 31, 2021, CDC will withdraw the request to the U.S. Food and Drug Administration (FDA) for Emergency Use Authorization (EUA) of the CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel, the assay first introduced in February 2020 for detection of SARS-CoV-2 only….. CDC encourages laboratories to consider adoption of a multiplexed method that can facilitate detection and differentiation of SARS-CoV-2 and influenza viruses."
Why masks on healthy persons? 40 plus years of “science” research by CDC saying masks do not work suddenly reversed. Why? Where is the “science” to wear a mask?
Actually the opposite: Harmful for children!!!!
https://jamanetwork.com/journals/jamapediatrics/fullarticle/2781743 (this is the study for above article)
https://www.aier.org/article/the-dangers-of-masks/
THE ABOVE ARTICLE WAS PUBLISHED ON JUNE 30, 2021 in JAMA, and retracted JULY 16- A peer reviewed article in one of America’s most prestigious journals. WHY?? WHAT IS GOING ON???? WHY WAS IT RETRACTED???
https://www.acpjournals.org/doi/10.7326/M20-6817
https://www.nejm.org/doi/full/10.1056/NEJMoa2029717
If you need more studies re: mask dangers please see Dr. Gaeta's letter with numerous references
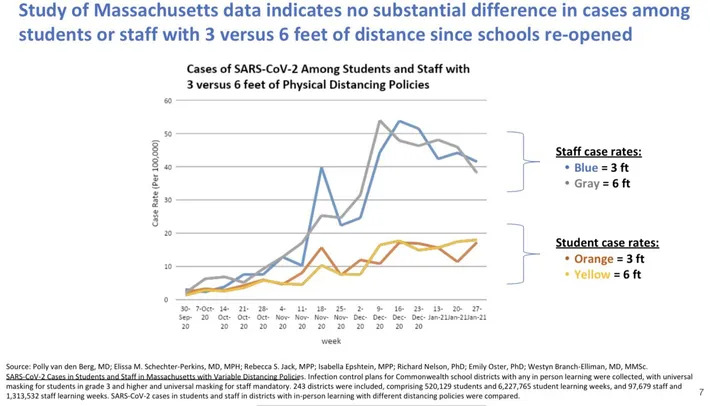
What about the 6 foot rule? No basis in science.
https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciab230/6167856
Why not a balanced approach to the “pandemic” ?
Why no early treatments, despite studies from 2005 showing chloroquine works?
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1232869/
Became apparent rather early on that if you waited to be hospitalized mortality increased to 25%.
Numerous “safe” treatments maligned. Why?
Actual campaign against early treatment. Why?
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31180-6/fulltext
Above article had to be retracted because it was false. Did the media ever correct the original reporting?
Who was and is behind the false data?
https://www.the-scientist.com/features/the-surgisphere-scandal-what-went-wrong--67955
Does early treatment work? Yes it appears so by anecdotal reports and unpublished studies. Different treatments with varying success.
Well known statically that if you get enough anecdotal reports that is equivalent to double blind placebo controlled studies. One knows the sun is shining despite the lack of a double blinded placebo controlled study.
https://www.nejm.org/doi/full/10.1056/NEJM200006223422506
Peru’s experience with Ivermectin:
https://dx.doi.org/10.2139/ssrn.3765018
Please watch:
https://vimeo.com/538598744/34f6104a08
***************************************************
June 17, 2021: DOUBLE BLIND STUDY!!!!!; Ivermectin works:
https://www.medrxiv.org/content/10.1101/2021.05.31.21258081v1
Unblinded study: https://medicalpressopenaccess.com/upload/1605709669_1007.pdf
https://www.sciencedirect.com/science/article/pii/S2052297521000792
Ivermectin mechanism of action:
https://www.nature.com/articles/s41429-021-00430-5
https://principia-scientific.com/breakthrough-ivermectin-inhibits-covid-spike-protein-binding/
https://pubmed.ncbi.nlm.nih.gov/32135219/
May 11, 2021
Dr. Zenlecko nominated for Nobel Peace Prize, but banned from US Social Media:
2 Kenyan Physicians speak out (one “allegedly” died of COVID after this interview):
https://www.bitchute.com/video/muHlkj4Emoep/
***************************************************
July 6, 2021:
LONG COVID: https://www.acpjournals.org/doi/10.7326/M21-0878
****************************************************************************
Treatment Studies(from Dr. Zelenko’s website):
1.https://www.sciencedirect.com/science/article/pii/S0924857920304258
2.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7365891/
3.https://pubs.acs.org/doi/10.1021/jf5014633
5.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7318306/
6.https://pubs.acs.org/doi/10.1021/jf5014633
7.https://www.sciencedirect.com/science/article/pii/S0924857920304258
9.https://www.nejm.org/doi/full/10.1056/NEJMoa2021436
10.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7392554/
11.https://www.medrxiv.org/content/10.1101/2021.01.26.21250494v1
September 2, 2021: Pfizer starts dosing patients in oral Covid-19 drug trial
Pfizer Inc started dosing its oral antiviral drug for Covid-19 in non-hospitalised, symptomatic adult patients.
ReutersNew YorkSeptember 2, 2021UPDATED: September 2, 2021 01:47 IST
News 24.5.2021 18:58 | updated 24.5.2021 18:58
This was 5-24-21:
Finnish firm earns US patent for Covid drug containing ivermectin and hydroxychloroquine
MAYBE IT WAS JUST THE “WRONG PEOPLE” FINDING A DRUG…..
3) COVID “Vaccines”
First Question: Is it appropriate to vaccinate in a pandemic?
Predicted the earlier you vaccinate the more mutations you get, so vaccinate against the virus , then vaccinate against the mutation that causes another mutation so you will need to vaccinate against that mutation and so on fueling the continued vaccine programs: great business model, but if you let heard immunity take place, minimal mutation, but no money to be made.
https://pubmed.ncbi.nlm.nih.gov/19022319/
Second Question: Are “specific” or “leaky”vaccines contributing the problem?
https://journals.plos.org/plosbiology/article/info:doi/10.1371/journal.pbio.1002198
Now read on:
Must consider the definition of vaccine and not confuse lay persons definition or understanding as to what constitutes a vaccine and how a lay person thinks a vaccine works.
Initially a vaccine was a weakened form of the virus/bacteria(antigen) or a dead form of it that was exposed to the person. As medicine “progressed” there were added vectors(something to carry the antigen) and adjutants(make the reaction stronger) to the mix. Sometimes the vectors and adjutants caused their own issues and complications rather than the virus or bacteria( antigen) that was trying to be immunized against. This is said to get one to understand that the vector or adjutant can be a problem itself just as the antigen of the disease.
Enter mRNA (vector)
MRNA is a new gene modifying therapy, similar to CAR-T and check point inhibitor therapy in oncology treatments, not a typical vector of carrying the antigen into the body. Rather it does not carry the antigen, but tells your own body to “make” the antigen. Once the body makes the antigen your own body then is supposed to recognize that it made something that is not human and “clean up” this mistake by making antibodies to this antigen it just made. If you think this is a round about process- I agree. It is said that this is much faster and cheaper than the old vector/antigen process to bring to market- I mean treatment.
Listen to the inventor of mRNA technology warn against mRNA: https://youtu.be/xC7_pRidnZ0 (if taken down by YouTube), try:
https://www.bitchute.com/video/OCCJpXVPj0eU/
Penn Medical Evaluation of mRNA: www.uphs.upenn.edu/cep/COVID/mRNA vaccine review final.pdf
JUNE 5, 2021: This goes into detail re: mRNA and the unknowns. A must watch for one to discuss intelligently the vaccine:
This is why you sign a release saying that it is experimental. Also why the US government is on the hook for damages rather than the drug companies.
There are numerous concerns with this gene modifying therapy from no successful animal experiments, other unintended immunological platform changes, and reverse transcription, to name a few. ( if you want a horror story please research these terms particularly in COVID use. Sleep well.)
Try These recent findings:
https://scivisionpub.com/pdfs/covid19-rna-based-vaccines-and-the-risk-of-prion-disease-1503.pdf
https://scivisionpub.com/abstract-display.php?id=1616
https://pubmed.ncbi.nlm.nih.gov/22095764/
SO: BLADE RUNNER VS THE WALKING DEAD
**********************************************************************
***********************************************************************
Enter COVID Spike protein(antigen)
Picking the antigen should be a well researched endeavor. The antigen could cause damage itself. If there is any cross reactivity with human tissues there can be issues of auto immune or other delayed sequela.
It is now known
https://www.sciencedirect.com/science/article/pii/S1537189120303281
https://www.qeios.com/read/26GTOD.2/pdf
https://sciencedirect.com/science/article/pii/S1092913420302288%20%E2%80%A6
https://doi.org/10.1161/CIRCRESAHA.121.318902
that the COVID spike protein regardless whether it is attached to a live virus or not causes endothelia damage. The very antigen that the rushed “vaccine” is having the body make. If you are slow to make antibodies is there a time period that the body will suffer damage? What if your body does not mount an adequate defense? What if you continue to make the spike protein?
Questions: Why such a rush to select the spike antigen?
Why not just a portion of the spike protein or another particle of the COVID virus?
If a medical doctor who rarely paid attention in immunology class grasped these concepts why would career immunologists not or did they?
Watch:
https://faculty.utrgv.edu/eleftherios.gkioulekas/presentations/2021-zelenko-protocol.html
**********************************************************************
June 11, 2021: This highlights my questions from above. Particularly re: epitome selection.
https://vrevealed.com/covid/webcast/james-lyons-weiler
**********************************************************************
Dangers being identified: DEATH RATE HIGHER THAN ALL OTHER VACCINES COMBINED, BUT YOU GET A FREE DOUGHNUT.
Death Count as of July 19, 2021 : 12,313 with 338 million injections= 1 death per 27,450 injections so assume 2 does per person (not taking into account the number getting the J&J vaccine) equals 1 death for every approximately 13,725 fully vaccinated. THIS IS PER VAERS WHICH IS UNDER REPORTED)

**ABOVE WAS POSTED July 20 with numbers through July 19, sometime between noon today July 21 and 3pm data was changed back to July 13 and only 6079 deaths WHAT IS GOING ON???????
CDC NOW SAYS THE POST WAS A MISTAKE YESTERDAY!!! They still have not updated the numbers through July, 19.
CDC website for adverse reports updated each week:
https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety/adverse-events.html
June 4, 2021
Harm from the vaccine is now being demonstrated without question despite the “small” numbers spin the media is trying to place on the story. Works out in Israel 1 in 2500 vaccinated males between ages 16-30 are developing myocarditis. Not a “small” number if you are in that age group:

Also: https://www.bitchute.com/video/Rd8BCXTow3Gq/
Watch: https://youtu.be/DNxoVFZwMYw
Finnish Legislator: https://rapsodia.fi/covid-vaccine-genocide-english-subtitles/
I didn’t know but the British government’s code name for the Pfizer injection prior to roll-out was “Ambush”
https://www.bmj.com/content/370/bmj.m3757/rr-3
June 11, 2021: “Urgent “ British Report Calls for Complete Cessation Of COVID Vaccines in Humans
This is a long but well written article:
https://www.technocracy.news/blaylock-on-vaccines-what-you-need-to-know-for-informed-consent
June 22, 2021: text portion - https://www.wsj.com/articles/are-covid-vaccines-riskier-than-advertised-11624381749
Reproductive organs at risk:
July 8,2021: Pfizer Tissue Distribution Study- please see pages 16 and 17 (English Version) Liver, Spleen, Adrenal, Ovaries: https://www.pmda.go.jp/drugs/2021/P20210212001/672212000_30300AMX00231_I100_1.pdf

July 8, 2021: “Japan: Another international group of physicians call for a stop.
"390 domestic doctors and 60 local council members agreed to the petition, and the founder, Toku Takahashi, Professor Emeritus of the University of Wisconsin Medical School (Director of the Clinic Toku), met in the Diet on the afternoon of the same day.
"The mortality rate is very low, and it is doubtful that all the people need to be vaccinated with a gene vaccine whose safety is still unknown, even though 80% of infected people are mildly ill." Other doctors who attended said that "the clinical trial has not been completed" and "at least 356 people have died after the vaccination"."”
https://www.sanspo.com/article/20210624-IOQJULJCVRMBXMZXIDJG6SDUHA/
On Sunday, July 11, 2021 at 9:39:42 AM UTC-7 Peter A. McCullough wrote:
10 Reasons to Drop Support or Mandates for Investigational COVID-19 Vaccines1. COVID-19 vaccination is voluntary research. The COVID-19 public vaccination program operated by the CDC and the FDA is a clinical investigation and under no circumstance can any person receive pressure, coercion, or threat of reprisal on their free choice of participation. Violation of this principle of autonomy by any entity constitutes reckless endangerment with a reasonable expectation of causing personal injury resulting in damages.
2. COVID-19 vaccines do not work well enough. The current COVID-19 vaccines are not sufficiently protective against contracting COVID-19 to support its use beyond the current voluntary participation in the CDC sponsored program. A total of 10,262 SARS-CoV-2 vaccine breakthrough infections had been reported from 46 U.S. states and territories as of April 30, 2021. Among these cases, 6,446 (63%) occurred in females, and the median patient age was 58 years (interquartile range = 40–74 years). Based on preliminary data, 2,725 (27%) vaccine breakthrough infections were asymptomatic, 995 (10%) patients were known to be hospitalized, and 160 (2%) patients died. Among the 995 hospitalized patients, 289 (29%) were asymptomatic or hospitalized for a reason unrelated to COVID-19. The median age of patients who died was 82 years (interquartile range = 71–89 years); 28 (18%) decedents were asymptomatic or died from a cause unrelated to COVID-19. Sequence data were available from 555 (5%) reported cases, 356 (64%) of which were identified as SARS-CoV-2 variants of concern, including B.1.1.7 (199; 56%), B.1.429 (88; 25%), B.1.427 (28; 8%), P.1 (28; 8%), and B.1.351 (13; 4%). None of these variants are encoded in the RNA or DNA of the current COVID-19 vaccines. In response to these numerous reports, the CDC announced on May 1, 2021, that community breakthrough cases would no longer be reported to the public and only those vaccine failure cases requiring hospitalization will be reported, presumably on the CDC website (https://www.cdc.gov/mmwr/volumes/70/wr/mm7021e3.htm).
3. The COVID-19 vaccines do not protect against the increasingly prevalent Delta variant. In the UK SARS-CoV-2 variants of concern report June 25, 2021, of 92,056 cases of delta, 42% were vaccinated.[i] Fortunately, among all Delta cases, there was a 0.3% mortality as compared to the alpha (UK) variant at 1.9%.
4. COVID-19 vaccines have a dangerous mechanism of action. The Pfizer, Moderna, and JNJ vaccines are considered "genetic vaccines" or vaccines produced from gene therapy molecular platforms.[ii] [iii] They have a injurious mechanism of action in that they all cause the body to make an uncontrolled quantity of the pathogenic spike protein from the SARS-CoV-2 virus. This is unlike all other vaccines where there is a set amount of antigen or live-attenuated virus. This means for the Pfizer, Moderna, and JNJ vaccines it is not predictable among patients who will produce more or less of the spike protein. The spike protein itself has been demonstrated to injure vital organs such as the brain, heart, lungs, as well as damage blood vessels and directly cause blood clots. Additionally, because these vaccines infect cells within these organs, the generation of spike protein within heart and brain cells in particular, causes the body's own immune system to attack these organs.
5. There is a burgeoning number of cases of myocarditis or heart inflammation among individuals below age 30 years.[iv] The Centers for Disease Control has held emergency meetings on this issue and the medical community is responding to the crisis and the US FDA has issued a warning on the Pfizer and Moderna vaccines for myocarditis.[v] It is known that myocarditis causes injury to heart muscle cells and may result in permanent heart damage leading to heart failure, arrhythmias, and cardiac death. Because this risk is not predictable and the early reports may represent just the tip of the iceberg, no individual under age 30 under any set of circumstances should feel any obliged to take this risk with the current genetic vaccines particular the Pfizer and Moderna products.
6. The US FDA has given an update on the JNJ vaccine concerning the risk of cerebral venous sinus thrombosis in women ages 18-48 associated with low platelet counts.[vi] Because this risk is not predictable no woman under age 48 under any set of circumstances should feel any obliged to take this risk with the JNJ vaccine.
7. COVID-19 vaccines are generating record safety reports. In 1990, the Vaccine Adverse Event Reporting Systems (“VAERS”) was established as a national early warning system to detect possible safety problems in U.S. licensed vaccines.[vii] VAERS is a passive reporting system, meaning it relies on individuals to voluntarily send in reports of their experiences to CDC and FDA. VAERS is useful in detecting unusual or unexpected patterns of adverse event reporting that might indicate a possible safety problem with a vaccine. The total safety reports in VAERS all vaccines per year up to 2019 was 16,320. The total safety reports in VAERS for COVID Vaccines alone through July 7, 2021 is 438,440.[viii]
8. People are dying and being hospitalized in record numbers in the days after COVID-19 vaccination. Based on VAERS as of June 25, 2021, there were 9,048 COVID-19 vaccine deaths reported and over 26,818 hospitalizations reported for the COVID-19 vaccines (Pfizer, Moderna, JNJ). By historical comparison, from 1999, until December 31, 2019, VAERS received 3,167 death reports (158 per year) adult death reports for all vaccines combined. Thus, the COVID-19 mass vaccination is associated with at least 57-fold increase annualized vaccine deaths reported to VAERS. COVID-19 vaccine adverse events account for 99% of all vaccine-related AEs from Dec 2020 through present in VAERS.
9. The safety profile is unknown and there is a reasonable expectation for harm for the following groups at all age ranges: COVID-19 recovered, suspected COVID-19 recovered, women of childbearing potential, children, persons with one or more chronic diseases.
10. Any personal choice or protected health information concerning the COVID-19 vaccine and its complications is confidential and anonymous according to federal law, otherwise, you will be subject to additional federal fines and penalties for violation of protected health information laws and statutes.
In conclusion, the investigational, genetic COVID-19 vaccines are not safe for general use and cannot be deployed indiscriminately unless proven otherwise. Please cease and desist pressure/harassment/mandates for COVID-19 vaccination.
[i]https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/997418/Variants_of_Concern_VOC_Technical_Briefing_17.pdf
[ii] To KKW, Cho WCS. An overview of rational design of mRNA-based therapeutics and vaccines. Expert Opin Drug Discov. 2021 May 31. doi: 10.1080/17460441.2021.1935859. Epub ahead of print. PMID: 34058918.
[iii] Doerfler W. Adenoviral Vector DNA- and SARS-CoV-2 mRNA-Based Covid-19 Vaccines: Possible Integration into the Human Genome - Are Adenoviral Genes Expressed in Vector-based Vaccines? Virus Res. 2021 Jun 1;302:198466. doi: 10.1016/j.virusres.2021.198466. Epub ahead of print. PMID: 34087261; PMCID: PMC8168329.
[iv] Abu Mouch S, Roguin A, Hellou E, Ishai A, Shoshan U, Mahamid L, Zoabi M, Aisman M, Goldschmid N, Berar Yanay N. Myocarditis following COVID-19 mRNA vaccination. Vaccine. 2021 Jun 29;39(29):3790-3793. doi: 10.1016/j.vaccine.2021.05.087. Epub 2021 May 28. PMID: 34092429; PMCID: PMC8162819.
[v] https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-june-25-2021
[vi] https://www.fda.gov/news-events/press-announcements/joint-cdc-and-fda-statement-johnson-johnson-covid-19-vaccine
[vii]VAERS may be publicly accessed at https://www.openvaers.com/covid-data.
[viii] VAERS may be publicly accessed at https://www.openvaers.com/covid-data (accessed July 9, 2021)
Changes to hide the facts,
From CHD news-release:
As more reports surface of breakthrough COVID cases, in and outside the U.S., the Centers for Disease Control and Prevention (CDC) today said it will change how breakthrough cases are reported, effective May 14.
According to a statement on the CDC’s website, the agency said to help “maximize the quality of the data collected on cases of greatest clinical and public health importance” it will stop reporting weekly COVID breakthrough infections unless they result in hospitalization or death.
The news followed another change, announced late last month, in how PCR tests should be administered to the fully vaccinated.
Both changes will result in lower overall numbers of reports of breakthrough cases in the U.S.
A breakthrough case is recorded if a person tests positive for SARS-Cov-2 two weeks after receiving the single-dose Johnson & Johnson (J&J) shot or completing the two-dose Moderna or Pfizer vaccination.
Why the changes matter
In April, the CDC issued new guidance to laboratories recommending reducing the RT-PCR CT value to 28 cycles — but only for those fully vaccinated individuals being tested for COVID.
In an RT-PCR test — the gold standard for detecting SARS-CoV-2 — RNA is extracted from the swab collected from the patient. It is then converted into DNA, which is then amplified.
CT, or cycle threshold, is a value that emerges during RT-PCR tests. A CT value refers to the number of cycles needed to amplify viral RNA to reach a detectable level.
According to the Indian Council of Medical Research, a patient is considered positive for COVID if the CT value is below 35. In other words, if the virus is detectable after 35 cycles or earlier, then the patient is considered positive.
Dr. Anthony Fauci recommends a CT value of 35. Globally, the accepted cut-off for CT value for COVID ranges between 35 and 40, depending on instructions from manufacturers of testing equipment.
“If the benchmark were to be lowered to 24 it would mean that CT values in the range 25-34 would not be considered positive,” according to the Indian Council of Medical Research, as reported by The Indian Express. “A benchmark of 35, therefore, means that more patients would be considered positive than we would get if the benchmark were 24.”
In other words, lowering CT threshold parameter may lead to missing infectious persons.
CDC won’t report new breakthrough numbers this week
Because the change in how the CDC will report breakthrough cases is still being implemented and won’t take effect until May 14, the CDC did not report new numbers this week.
According to the latest available numbers, as of April 26, the CDC reported 9,245 people had tested positive for COVID at least two weeks after getting their final COVID vaccination. About 9%, or 835, people required hospitalization and 132 died.
Of the hospitalized patients, 241 were said to be asymptomatic or having an illness not related to COVID, and 20 deaths were reported as asymptomatic or not related to the disease.
The latest numbers are from 46 U.S. states and territories. It’s not clear which four states didn’t submit breakthrough case figures to the CDC.
“These surveillance data are a snapshot and help identify patterns and look for signals among vaccine breakthrough cases,” the CDC said in an April 27 statement. “As CDC and state health departments shift to focus only on investigating vaccine breakthrough cases that result in hospitalization or death, those data will be regularly updated and posted every Friday.”
According to the CDC, actual vaccine breakthrough numbers are likely higher as the surveillance system is passive and relies on voluntary reporting from state health departments and may not be complete. In addition, some breakthrough cases will not be identified due to lack of testing. This is particularly true in instances of asymptomatic or mild illness, CDC added.
The CDC said vaccines are still effective, noting the breakthrough cases represent a small percentage of those who have been vaccinated.
****************************************************************
June 10, 2021: More Studies Confirming: IF YOU HAVE HAD COVID YOU DO NOT NEED A VACCINE. IT MAY BE HARMFUL.
https://www.medrxiv.org/content/10.1101/2021.06.01.21258176v2
https://www.sciencedirect.com/science/article/pii/S0092867420310084
https://www.medrxiv.org/content/10.1101/2021.01.15.21249731v2.full.pdf
https://www.aier.org/article/if-you-had-covid-do-you-need-the-vaccine/ (summary article)
July 6, 2021: Natural immunity better against COVID mutations than “vaccines”: https://www.medrxiv.org/content/10.1101/2021.07.01.21259833v1.full.pdf
July 15, 2021: For those of us exposed to COVID and wondering why we have not become symptomatic:
https://doi.org/10.3390/v13060961
What about re-infections with COVID virus? Is it common? Cellular T-cell immunity?
No! We have looked at the published evidence and can conclude based on the existing body of evidence, that reinfections are very rare, if at all and based on typically one or two instances with questionable confirmation of an actual case of re-infection e.g. flawed PCR testing etc. (references 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26). A very recent study in Qatar (Lancet) found that “natural infection appears to elicit strong protection against reinfection with an efficacy ~95% for at least seven months”. Hall in Lancet reported same. “The study in Austria also found that the frequency of re-infection from COVID-19 caused hospitalization in only five out of 14,840 (0.03%) people and death in one out of 14,840 (0.01%)”.
Dr. Marty Makary of Johns Hopkinswrote “reinfection is extremely rare and even when it does happen, the symptoms are very rare or [those individuals] are asymptomatic”.
Importantly, the World Health Organization (WHO) has recently (May 10th 2021 Scientific brief, WHO/2019-nCoV/Sci_Brief/Natural_immunity/2021.1) alluded to what has been clear for many months (one year now), which is that people are very rarely re-infected. The WHO is very late but better late than never. The key points they have stated in this briefing which stand out and warrants a mention (again we always knew this and tried informing the CDC and WHO of this across the last year) is that:
i) Within 4 weeks following infection, 90-99% of individuals infected with the SARS-CoV-2 virus develop detectable neutralizing antibodies.
ii) Available scientific data suggests that in most people immune responses remain robust and protective against reinfection for at least 6-8 months after infection (the longest follow up with strong scientific evidence is currently approximately 8 months).
iii) Studies aimed to detect immunological memory including the assessment of cellular immunity by testing for the presence of memory B cells, and CD4+ and CD8+ T cells, observed robust immunity at 6 months post-infection in 95% of subjects under study, which included individuals with asymptomatic, mild, moderate and severe infections.
iv) Current evidence points to most individuals developing strong protective immune responses following natural infection with SARS-CoV-2.
A very recent discussion on mild COVID-19 inducing lasting antibody protection, was based on a publication in Nature. The research showed that people who have had mild illness develop antibody-producing cells that can last a lifetime. “Months after recovering from mild cases of COVID-19, people still have immune cells in their body pumping out antibodies against the virus that causes COVID-19, according to a study from researchers at Washington University School of Medicine in St. Louis. Such cells could persist for a lifetime, churning out antibodies all the while”.
We also wish to re-iterate the accumulated strong evidence that prior infection with other coronaviruses and common cold coronaviruses confer cellular immunity via T-cell immunity etc. (Weiskopf , Grifoni, Le Bert, Mateus, Tavukcuoglu,Cassaniti, Dykema, Echeverría,Bonifacius, Nelde, Ansari, Ma, Lineburg, Borena) (references 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14).
Indeed, the evidence now abounds that SARS-CoV-2-reactive CD4+ T cells as an example, are seen in unexposed individuals, suggesting preexisting cross-reactive T cell memory. “A positive response was observed up to 12 months after COVID-19 infection (median 246 days after symptom onset; range 118-362 days)… long-term SARS-CoV-2 T-cell response might accompany a waning humoral response”. Of note, SARS-CoV-2 T-cell response seems to be mainly mediated by CD4 T cells. This immunity appears also to be long-lasting e.g. SARS-1 has remained for 18 years. Of 23 patients who had SARS-1 in 2003, researchers found all 23 retained memory T cells induced by the parental SARS-1 pathogen in their systems after 17 to 18 years. Moreover, when they looked at convalescent SARS-CoV-2 patients (n=36), they uncovered that the 36 had also produced similar memory T cells.
“Results suggest that following a typical case of mild COVID-19, SARS-CoV-2-specific CD8+ T cells not only persist but continuously differentiate in a coordinated fashion well into convalescence, into a state characteristic of long-lived, self-renewing memory”.
In early March 2020, a SARS-CoV-2 outbreak in the ski resort Ischgl in Austriainitiated the spread of SARS-CoV-2 throughout Austria and Northern Europe. Follow-up shows that although antibodies to SARS-CoV-2 declined, T and B cell memory can be detected for up to 8 months.
A recent publication in Nature indicates that SARS-CoV-2 infection induces long-lived bone marrow plasma cells in humans. Researchers found in 77 patients with mild infection, consistently there was circulating resting memory B cells directed against the S protein and detected in the convalescent individuals. They demonstrated that “in patients who experienced mild infections (n=77), serum anti-SARS-CoV-2 spike (S) antibodies decline rapidly in the first 4 months after infection and then more gradually over the following 7 months, remaining detectable at least 11 months after infection. Anti-S antibody titers correlated with the frequency of S-specific BMPCs obtained from bone marrow aspirates of 18 SARS-CoV-2 convalescent patients 7 to 8 months after infection”.
Overall, the research showed that SARS-CoV-2 infection induces a robust antigen-specific, long-lived humoral immune response in humans.
One very important piece of research emerged when researchers studied the blood of older people who survived the 1918 influenza pandemic. The research group collected blood samples from 32 pandemic survivors aged 91 to 101. “The people recruited for the study were 2 to 12 years old in 1918 and many recalled sick family members in their households, which suggests they were directly exposed to the virus, the authors report. The group found that 100% of the subjects had serum-neutralizing activity against the 1918 virus and 94% showed serologic reactivity to the 1918 hemagglutinin. The investigators generated B lymphoblastic cell lines from the peripheral blood mononuclear cells of eight subjects. Transformed cells from the blood of 7 of the 8 donors yielded secreting antibodies that bound the 1918 hemagglutinin”.
Additionally, Antia and colleagues looked at heterogeneity and longevity of antibody memory to viruses and vaccines. Their results found that “some individuals have, on average, slightly longer-lasting memory than others—on average, they have higher antibody levels with slower decay rates. We identified different patterns for the loss of protective levels of antibodies to different vaccine and virus antigens. Specifically, we found that for the first 25 to 50 years, virtually all individuals have protective antibody titers against diphtheria and tetanus, respectively, but about 10% of the population subsequently lose protective immunity per decade. In contrast, at the outset, not all individuals had protective titers against measles, rubella, and vaccinia. However, these antibody titers wane much more slowly, with a loss of protective immunity in only 1% to 3% of the population per decade. Our results highlight the importance of long-term longitudinal studies for estimating the duration of protective immunity and suggest both how vaccines might be improved and how boosting schedules might be reevaluated”.
Researchers have also opined that the cytokine storm seen in COVID-19 is mediated by a para (personal communication Dr Hamid A Merchant BPharm MPharm PhD RPh CQP PGCertHE FHEA SRPharmS)“cholinergic epitope on the spike activating macrophages leading to cytokine storm”. They go on to argue that this is the hidden secret (a sort of double-edged sword) explaining how the virus deregulates the immune response at one end and keeps mutating the S1 so as to enable better binding affinities to ACE2 and evade the immune response. Para “Using full spikes encoding in genetic vaccines. We now know that spikes can be freely circulating post-CoViD vaccines, this can explain the emergence of new variants”. The authors go further with a possibility that para “the vaccines itself might facilitate recombinant mutations”. “For example, if people in India are inoculated with vaccines that encode the spike of a variant from outside India, say UK, the local strains are now exposed to strains from the UK”.
In closing, we also argue that if you are re-infected, it is most likely not with the initial parental strain you were infected with and most likely with a variant. Moreover, had you developed natural exposure immunity, this is usually very robust and durable and will safeguard against variants/mutants. There are many questions at this time as to the ability of the very narrow ‘spike-specific’ immunity (spike epitopes) conferred by the mRNA and adenovirus vector delivery platforms. It is possible and highly probable that variants could blow past the existing vaccines and we are seeing this today whereby doctors report that 60% of the new COVID infections already have had both vaccination shots.
This phenomenon post vaccination warrants urgent focus by authorities and study. We also are witnessing a phenomenon whereby the immune system is depressed for approximately two weeks post vaccination with evidence of lymphopenia, leucopenia, and neutropenia. Elderly and high-risk persons must be warned about this during the informed consenting phase so that they can take precautions to not be exposed for two to three weeks post vaccination.
**************************************************************************
For those who took a COVID “vaccine” and are having issues:
OTC Medicines & Nutraceuticals to Prevent/Reduce COVID Post-Vaccination Side Effects These recommendations are based on the clinical experience of COVID-expert doctors surveyed. The recommendations are designed to address two concerns:
1. Prevention or reduction of side effects and adverse events that may in some cases be severe. The schedule for each nutraceutical or medicine is designed to cover the time when various of the side effects have been reported. 2. “Breakthrough” COVID infection is being reported during the approximately two weeks before immunity from the vaccine starts. The recommended antivirals and vitamin D help protect against these shortly-after-vaccine COVID infections. Vitamin D also helps protect against vaccine side effects. All the therapeutics listed are available over the counter without prescription. However, for those with access to them, adding ivermectin or hydroxychloroquine enhances the anti-COVID protection. Ivermectin for protection against COVID infection is recommended at a dosage of 0.2 mg/kilogram of body weight (typically around 12 - 18 mg/dose). An often cited protocol is to take one dose, then after 48 hours take a second dose. Then take once per week. Hydroxychloroquine for protection against COVID infection is often recommended at 200 mg once a day for 5 days, then 200 - 400mg one time a week.
Aspirin (anti-thrombotic) 325 mg/day for 4 weeks beginning the day before vaccination.
Ibuprofen (anti-inflammatory) Two 200 mg caplets 3 times/day the day before, day of and day after vaccination. Continue as needed if symptomatic (fever, muscle aches, headache, etc.)
Loratadine (Claritin or generic equivalent; H1 blocker, anti-inflammatory) 10 mg/day the day before, day of and day after vaccination.
Famotidine (Pepcid or generic equivalent; H2 blocker, anti-inflammatory) 20 mg twice per day the day before, day of and day after vaccination. (not Prilosec or other PPIs)
Vitamin D3 (potent anti-inflammatory effects at sufficient dosage; anti-viral immune enhancement) One dose of 50,000 IU five to seven days before vaccination (serum levels peak on average at 7 days), Then daily 15,000 IU until 5 days after vaccination, Then continue with maintenance dosage of 5,000 - 10,000 IU/day.
For extra protection against breakthrough COVID infection during the approximately two-week window before immunity starts:
Zinc (anti-viral) 50 mg/day started as far ahead of vaccination as possible and continued three weeks or indefinitely.
Quercetin (zinc ionophore, to enhance zinc anti-viral effect; anti-inflammatory; anti-thrombotic) 250 mg twice per day for three weeks starting the day before vaccination.
Vitamin C (anti-viral; anti-inflammatory) 3,000 mg/day started as far ahead of vaccination as possible and continued three weeks or indefinitely.
DISCLAIMER: This information is for educational purposes only. It is not intended to serve as a substitute for diagnosis, treatment, or advice from a qualified, licensed medical professional. Any treatment you undertake should
************************************************************
*************************************************************
June 11, 2021: China now has the “old” style vaccine and are vaccinating at warp speed. 20 million doses a day. WHY CANNOT WE HAVE THE “OLD STYLE” ?
China’s production capacity is especially noteworthy given that both CoronaVac and the Sinopharm vaccine are made from inactivated virus.Scientists say that vaccines of this type require more time and effort to produce than do COVID-19 vaccines based on mRNA technology, such as thePfizer or Moderna shots. To produce killed virus, manufacturers first need to grow it in living cells in large bioreactors, which can take months, explains Kis.
To achieve its massive gains, China probably leveraged its existing capacity for manufacturing inactivated-virus vaccines against other diseases, including influenza and hepatitis A, says Jin Dong-Yan, a virologist at the University of Hong Kong.
************************************************************
Good Source of general info and school mandate info: https://childrenshealthdefense.org/
Resource if your child or you are facing a school vaccine mandate: https://www.tpusa.com/vax
Strongly consider changing schools, taking a year off, etc. -nothing talks better than schools losing monies!!!!
June 17, 2021:
Open Letter:
June 17, 2021
COVID-19: Is College Worth the Risk of the Shot?
Are you one of the millions of American students (or their parents) facing the choice of taking the COVID shot or being barred from school?
The 800 reported cases of heart inflammation, now being investigated by the Centers for Disease Control and Prevention (CDC), give a new urgency to the question. The most poignant casemight be the 19-year-old girl, a journalism student at Northwestern University, who died two months after receiving her first dose of the Moderna product. Even a heart transplant could not save her.
One of the world’s most widely published cardiologists, Dr. Peter McCullough, fears that many of these formerly fit and healthy young people will wind up with heart failure.
Depending on the amount of underreporting, the rate of heart problems in young men following the COVID jab may be 600 times the background rate.
Half the patients with a diagnosis of heart failure live less than 5 years. Even if heart damage is mild, the patient might not be able to participate in athletics or aspire to be a pilot, firefighter, or soldier, or to engage in any physically demanding occupation.
Another potential risk is infertility. This might not become apparent for years, as college students are generally postponing childbearing until they achieve educational or career goals. But an early warning signal is coming from fertility clinics, where eggs and sperm from previously successful donors are not producing viable embryos.
Having a significant fraction of our young people disabled or infertile is a truly existential risk.
Yet, despite objections from physicians, hundreds of colleges are still insisting that students get the jab, even those already immune, who gain no conceivable benefit.
Legal challenges may be undertaken, but courts have generally been unsympathetic to challenges to vaccine mandates. A Texas court just dismissed a challenge by some 116 employees of the Houston Methodist hospital system, who will be fired if they decline the shots.
Many will take the shots, even against their better judgment, because of peer pressure, continued trust in the CDC, the belief that these genetically engineered products are no different from other vaccines, or the high cost of disrupting their career plans. Since the purveyors of the products are protected from liability, all costs—even of death and disability—will be borne by students and their families.
For further information:
· Weekly summaries of reports to British Yellow Card system(scroll down to “vaccine analysis print” for the various brands)
Contact jane@aapsonline.org or (520) 323-3110 if you would like to discuss these issues.
Jane M. Orient, M.D Executive Director, Association of American Physicians and Surgeons
“ VACCINE” HARMS
https://ard.bmj.com/content/early/2021/07/22/annrheumdis-2021-220647
There were no postvaccination symptomatic cases of COVID-19 among patients with AIIRD and one mild case in the control group. Major adverse events in patients with AIIRD included death (n=2) several weeks after the second vaccine dose, non-disseminated herpes zoster (n=6), uveitis (n=2), and pericarditis (n=1). Postvaccination disease activity remained stable in the majority of patients.
Conclusion mRNA BNTb262 vaccine was immunogenic in the majority of patients with AIIRD, with an acceptable safety profile. Treatment with glucocorticoids, rituximab, MMF, and abatacept was associated with a significantly reduced BNT162b2-induced immunogenicity.
DOES 2 DEATHS, 6 NON-DISSEMINATED HERPES ZOSTER, 2 UVEITIS, AND 1 PERICARDITIS OUT OF 686 PATIENTS SEEM LIKE AN ADEQUATE SAFETY PROFILE? DOUBLE CHECK WHAT ARTICLES “CONCLUDE”.
September 29, 2021: Death rates in Israel parallels vaccination rates:
https://boriquagato.substack.com/p/israeli-booster-shotdeaths-update
October 1, 2021: Patients with cerebral venous sinus thrombosis after SARS-CoV-2 vaccination who met criteria for thrombosis with thrombocytopenia syndrome had a distinct clinical profile and high mortality rate.
https://jamanetwork.com/journals/jamaneurology/fullarticle/2784622
PREGNANCY:
You can reference the original NEJM article from this article, but I liked the explanation this article gives and shows intellectual dishonesty (this is the infamous Table 4 and if your doctor does not know about this-shame on them):
THEY Finally added a correction to the NEJM article(did this get publicized?):
https://www.nejm.org/doi/full/10.1056/NEJMx210016
Certain antibodies make the illness worse:
https://www.biorxiv.org/content/10.1101/2020.12.18.423358v1
EUROPEAN ADVERSE REPORTING SITE:
https://www.adrreports.eu/en/search_subst.html#
CDC website for adverse reports updated each week:
https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety/adverse-events.html
WHAT ARE THE LONG TERM SIDE EFFECTS OF THE “VACCINES” ? WE DO NOT KNOW YET, BUT some additional complications rather than just blood clots:
https://www.pnas.org/content/118/21/e2105968118
https://www.scivisionpub.com/previous-display.php?journal=svjmi&&v=5&&i=4&&y=2021&&m=August
“ VACCINE “ EFFICACY
July 30,2021: CDC Alarmed 74% of Cape Cod Cluster Vaccinated
The above was predicted(see below) and answers Question 1 from above:
mRNA and the vector COVID vaccines are “leaky ” i.e., do not stop infection or transmission. In a dramatic appeal to the WHO: top virologist Geert Bossche warned of deaths from mass corona vaccinations (Epoch Times March 2021) because leaky vaccines encourage the mutation and spread of more infectious viral variants. In May, world-reknowned Nobel laureate virologist Montagnier agrees. Thus, vaccinated persons become spreaders of more infectious mutations of SARS-COV-2. The more people vaccinated, the higher the risk of evolving strains. There is evidence of vaccinated spreaders, with an increase in serious COVID cases among the young, e.g. in Israel. "Break-through" cases are occurring in fully vaccinated people worldwide. E.g., Florida;
INCREASE IN COVID CASES and VARIANTS PARALLELS VACCINATION (this was predicted as above and is being proven by the European data):
VACCINATION DURING AN OUTBREAK CAUSES MUTATIONS -Epidemiology 101

ISRAEL AND UK DATA:
http://www.kathydopp.info/node/66
September 7, 2021:
Israel Data
September 7, 2021: English Data:
CDC moves goalposts when determining COVID-19 breakthrough cases
IF vaccinated more likely to get Delta:
CDC moves the GOALPOSTS AGAIN:
http://epmonthly.com/article/crash-cart-drinking-cow-urine-prevents-covid/
Welcome to life in a pandemic when big business and government make medical decisions. Let’s ratchet up the cycle thresholds for COVID testing for those getting the virus without the vaccine and ratchet down the cycle thresholds for those already vaccinated. I believe the vaccines work in reducing mortality, however, is this simply a move to bolster public confidence in the effectiveness of vaccines?
—Salim R. Rezaie, MD
I’m surprised that we clinicians are rather accepting of the fact that government science experts would manipulate results to sustain a public narrative that is not founded in fact. Shouldn’t we be forcing this out into the mainstream of public discussion? If we don’t, the truth will finally come out and we will look like we have been complicit in a government misinformation campaign.
– Mark Plaster, MD, JD
Lowering the cycle threshold of testing in “only” those patients who received a vaccination to make it harder to declare COVID positivity in that patient subset is unscientific, unethical and deceitful. Talk about “moving the goalposts.” If the CDC is distorting this data, what other data is it distorting and why? A better question is why the medical establishment isn’t objecting to the CDC’s actions.
– William Sullivan, DO, JD
***********************************************
“Is there any way to square the American data, supposedly showing that 99% of the hospitalized are unvaccinated, with the data from e.g. the UK and Israel, showing vaccinated make up anywhere from 40%-60% (roughly half) of the hospitalized? Are they literally now treating two different diseases? Conversely, is it really possible to cook the books in this country to such an extreme extent? See Israeli data below, also Israeli study showing vaccine is only 39% effective at stopping transmission(!)”
THE FOLLOWING IS FROM AN EMAIL THREAD OF PEOPLE EXTREMELY SMART and copied with permission without identification of the individuals:
I'm not sure if these will answer your questions or not. However,
(1) the COVID vaccine trials only estimated the "RELATIVE" effectiveness that ignores:
(a) the number of the vaccinated and placebo participants, and
(b) the prevalence of the disease (COVID-19), and
(c) the difference in the percentages of vaccinated versus placebo group who became ill with the disease (COVID-19)
(2) the ABSOLUTE effectiveness shown in the Pfizer vaccine trials (using a healthier, lower risk, group than the vaccines were rolled out on) show:
(a) 0.0368% = 1/2717 i.e. it takes vaccinated 2,717 persons to reduce one (1) serious COVID case.
(b) the increased Absolute risk of vaccine adverse events is 15.6% which means 424 of every 2717 people are expected to have adverse events for each one (1) person without a serious COVID case.
(c) the increased risk of SERIOUS vaccine adverse events is 0.4653 % which means 13 of every 2717 people vaccinated are expected to have adverse events for each one (1) person without a serious COVID case.
(d) This is despite the fact that 251 more people in the vax'd group were mysteriously eliminated from the trial calculations post-full-vaccination, than in the placebo group (because of serious adverse reactions? we are never told).
You can see the calculations here for Pfizer and the same results for Moderna and Jannsen
(3) Empirically, the data from the UK, Israel, and Iceland (unavailable in the US) show NO positive effect at reducing COVID cases, hospitalizations, or deaths for the vaccinated within 2 months after vaccination. In Israel, the vaccine administrator now wants to vaccinate the entire population 6 times/year or every 2 months.
(4) Death rates in the elderly have risen during vaccination rollouts targeting the elderly population.
Dramatic increase in COVID Deaths coincides with COVID vaccine rollouts
(5) The rise of the Delta virus is concomitant with the vaccine rollouts. Gerrt Bossche and Luc Montagnier both predicted immune escape of using leaky COVID vaccines would cause viral escape and more infectious mutations to mutate in and be spread by the vaccinated, as appears to be the case today. Search for some of their works on:
Scientists and Doctors Warn Against investigational COVID-19 Vaccines
The US CDC, hospitals,... are not tracking the vaccine status of COVID patients today and are manipulating the numbers:
The truth about vaccines that the CDC doesn’t want you to know. July 11, 2021 The CDC has announced and encouraged asymmetric testing and reporting. Specifically they [CDC] are advising no asymptotic testing on vaccinated and continued testing on unvaccinated to generate more false positives and drive up the case count in the unvaccinated. At the end of May, after flooded with >10,000 manually confirmed vaccine failures, the CDC gave up tracking and stated they will no longer count vaxxed in case count. So the reports of 99% of cases in unvaxxed are false. Data from Israel and UK suggest the percent cases in vaxxed and unvaxxed will match the population prevalence of vaxxed. ...But what both Dr. Vivek Murthy and Press Secretary Jen Psaki neglect to say is that the biggest misinformation is coming from the CDC, FDA, and NIH. Those organizations do not want you to know how many people have been killed or permanently disabled by the COVID vaccines. And they want you to believe that early treatments don’t work.
CDC Caught Cooking the Books on COVID Vaccines. Analysis by Dr. Joseph Mercola Fact Checked. June 11, 2021.Now, as over 100 million Americans have been “vaccinated” against COVID-19, the CDC is lowering the CT from 40 to 28, but only when diagnosing vaccine breakthrough cases — cases where fully vaccinated individuals are diagnosed with COVID-19To make matters worse, the CDC also will no longer record mild or asymptomatic infections of those who were immunized as “COVID cases.” The only cases that now count as COVID cases for someone immunized with the COVID-19 vaccine are those that result in hospitalization or deathCaught Red-Handed: CDC Changes Test Thresholds To Virtually Eliminate New COVID Cases Among Vaxx'd. May 21, 2021 Outcome Reporting Bias in COVID-19 mRNA Vaccine Clinical Trials. January 2021. by Ronald B. Brown. School of Public Health and Health Systems, University of Waterloo, Waterloo, ON N2L3G1, Canada. Relative risk reduction and absolute risk reduction measures in the evaluation of clinical trial data are poorly understood by health professionals and the public. The absence of reported absolute risk reduction in COVID-19 vaccine clinical trials can lead to outcome reporting bias that affects the interpretation of vaccine efficacy. ... Absolute risk reduction in the Pfizer trials was only 0.7%. For Moderna trials, the absolute risk reduction was only absolute risk reduction, 1.1%. USA: Post-vaccination increase in all-cause mortality
In the US, all-cause mortality has been increasing in many younger age groups since about March/April 2021, despite a significant decrease in covid deaths since January.
With all that above in mind, I would say that the actual effectiveness of COVID vaccines is less than nil since doctors seem to be now reporting treating more COVID-vax'd patients for COVID and for COVID vaccine injuries, than the number of unvaccinated COVID patients.
Sadly I don't think it will matter. They are going to shove this thing through. The FDA just approved an alzheimers drug despite every single person on the panel voting against it because it caused brain swelling in 40% of patients. What's a few elderly people more or less? It's just awful.
Among the various science classes and labs in college I was obliged to also take several courses in statistics. It was a long time ago, so just checking with others.
We’ve all heard the claims trumpeted in the media of 95% effective, 91% effective, even 99% effective— but what does that really mean? I don't think it really means what it is purported to mean.
The clinical trials of course use endpoints, both primary and secondary, to measure efficacy (in a controlled environment) and safety. The endpoints can be generally concerning (a) prophylaxis (prevention), (b) reducing the severity of the disease itself including symptoms, or for (c) shedding/transmission. Different jab manufacturers can choose different endpoints to measure the efficacy of their own concoctions as allowed by the FDA.
There are however some FDA applicable guidelines. For viruses and specifically the COVID-19 disease, FDA guidelines recommend minimal phase 3 success criteria for approval of a vaccine as follows: an estimated reduction in the primary endpoint (whatever that endpoint is determined to be) of at least 50% in the vaccine group versus the placebo group, with a 95% CI (confidence interval) providing assurance of at least a 30% reduction (as consistent with WHO trial design) of a given endpoint/symptom group, and the acceptable primary endpoints for approval could include SARS-CoV-2 infection, symptomatic infection (COVID-19), severe COVID-19, or some combination of these.
What is being reported appears to be this: to be approved, a vaccine must assure that at least 50% of a vaccinated/jabbed group— in comparison to an unvaccinated group, shows at least a 30% reduction of a given primary endpoint with a 95% certainty that the population mean is within these numbers. 95% confidence interval it would appear does not mean "there's only a 5% chance that I'll contract COVID-19 if I get the vaccine."
If this is correct, even a jab deemed statistically "effective" may be far from it in real-world terms.
I further read that people in the know agree that is will be practically impossible to determine effectiveness of vaccine effects for prevention of severe COVID-19 or death (the only endpoints that really matter) until a phase 4 trial involving a great number of people can be completed which will take many years. The only other actual disease-related endpoints measurable at present are mild to moderate COVID-19 symptoms.
Is my understanding of the statistics involved correct?
USING CDC NUMBERS THE VACCINE CAUSES MORE HARM THAN COVID TILL AGE 50 ( SEE BELOW):

4) Treatment
September 11, 2021: What is the US doing wrong?
Even Guatemala does a better job:
https://mobile.twitter.com/ontkenningsfase/status/1440389474991558665?s=21
Go to these websites and connecting websites for general overview and research of treatment :
What not to take: https://www.nejm.org/doi/full/10.1056/NEJMoa1910993
Remdesivir causes multi-organ failure(kidney), pulmonary edema, hypotension—sounds like COVID — Remdesivir had a 53% mortality when tried on EBOLA—this medicine is toxic.
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31022-9/fulltext
https://www.covid19treatmentguidelines.nih.gov/tables/table-2a/
5) PSYCHOLOGY
“Pandemic” Playbook taken from Brave New World( Aldous Huxley-teacher) and 1984(George Orwell-student)
President Eisenhower warned :
“Yet, in holding scientific research and discovery in respect, as we should, we must also be alert to the equal and opposite danger that public policy could itself become the captive of a scientific-technological elite. It is the task of statesmanship to mold, to balance, and to integrate these and other forces, new and old, within the principles of our democratic system-ever aiming toward the supreme goals of our free society.”
*****************************************************************
The “GROUP THINK” of our citizens is beyond disturbing. Rather than be appreciative of people questioning unscientific mandates, society would rather attack the critical thinkers. It is summarized by another physician in this manner:
“I agree that most physicians and the general public appear to be in a hypnotic state of sorts. This has happened before throughout history so we can’t blame it entirely on the media although I do think that the media/ social media have played a huge role in accentuating this human tendency. I would like to see a study comparing physician’s views on the COVID-19 vaccines with how much time they spend on Facebook or watching TV.
I’ve also likened our collective behavior to a stampede. Stampedes are driven by fear in response to some threat, whether real or imagined. In a stampede, each herd animal is judging its pace, direction and position in the herd relative to its neighboring animals rather than any objective measure outside of the herd. It doesn’t matter if the herd is heading over a cliff. All that matters to each animal is that they are maintaining their position within the herd. You would think humans could transcend that kind of low -level thinking, and some do. But the majority of humans function as herd animals, even more so when they are fearful (even though I believe we all have the potential for transcendence).
The group think mentality that drives us to stampede is inherent to our nature to an extent. However, there are factors that can amplify that tendency. Some have speculated that our brain functioning is impaired by modern environmental toxins. Like the Romans suffering from lead poisoning at the fall of their empire, most Americans don’t even seem to care that the “barbarians are at the gates”. Historians may speculate that the chemicals in our food, water and air were contributing factors. Perhaps years of non-regenerative agriculture lead to the soil depletion of key nutrients needed for optimal cognitive function. And who knows what 5G is now doing to many of our brains? Certainly nothing good.
Of course, we’ve known for decades the Marxists have been hard at work eroding our educational system. When teenagers graduate high school without knowing how to read or solve a basic mathematical equation, what could we expect? We haven’t been teaching children to be critical thinkers for quite some time, maybe generations. “
Excellent Analysis of above:
https://europepmc.org/article/PPR/PPR295537
Peer Pressure:
https://www.jennifermargulis.net/covid-vaccine-peer-pressure/
Eric Clapton addresses “emotional blackmail”:
Pessimist View:
https://consentfactory.org/2021/06/20/manufacturing-new-normal-reality/
On a lighter note here is Bill Maher on COVID- notice this is R rated from his show, but with valid points.
https://www.youtube.com/watch?v=Qp3gy_CLXho
May 8, 2021
Interviews worth watching with Holocaust Survivor (puts everything in perspective):
https://www.youtube.com/watch?v=PdlWhuUFuKs
What is going on? https://www.lewrockwell.com/political-theatre/dr-peter-mccullough-important-longer-video/
Russell Brand sums it up (it is not and never was about your good health):
July 6, 2021: Summary of events and dangers (Crimestop and protective stupidity) :
AND IF YOU CANNOT ARTICULATE FACTS, JUST CENSOR THE FACTS OR THE SPEAKERS: (you may not agree with what is said, but the person must be allowed to speak- as Galileo said “I have never met a man so ignorant that I couldn't learn something from him”)
How to conduct propaganda:
CONTROL THE NARRATIVE(even if you have to lie):
What might have been:
An Alternate COVID-19 Reality
Raphael B. Stricker, MD
Labor Day 2021
We are now 21 months into the COVID-19 pandemic with over 200 million SARS-CoV-2 infections and 4 million deaths worldwide. What follows is a fantasy of what could have happened if the pandemic had been addressed with integrity, intelligence and competence instead of stupidity, hubris and greed.
November 2019: A viral escape from the Wuhan Institute of Virology results in numerous infections. Although initially the escape is considered containable like similar lab escapes in Beijing and Guangdong, the number of cases continues to rise. The Chinese Communist Party (CCP) informs the world about the mishap in December 2019.
January 2020: The first cases of COVID-19 are reported in the USA and other countries. Cases on cruise ships follow. The Trump administration cuts off travel from China.
February 2020: The studies of Zelenko and Raoult et al. show that hydroxychloroquine (HCQ) is effective against SARS-CoV-2. President Trump endorses HCQ.
March 2020: The Indian Council of Medical Research (ICMR) proposes a regimen for pre-exposure prophylaxis (PrEP) of COVID-19 using weekly HCQ. Studies begin in India using this regimen in high-risk healthcare workers. The Trump administration mobilizes its HCQ stockpile.
April 2020: Cases rise in the New York metropolitan area. The Trump administration issues an order to distribute HCQ for weekly PrEP. More than 70 million doses are given to nursing home patients and outpatients across the USA. A World War II-style stockpile enhancement produces 500 million more doses of HCQ.
May 2020: The CDC explores production of a COVID-19 vaccine. Pharma companies report that a fully-tested vaccine would not be available until 2024. Early treatment of COVID-19 with antibiotics is given top priority to keep patients out of the hospital.
June 2020: The number of COVID-19 cases plateaus in the USA as HCQ PrEP broadens. The India studies show promise for the weekly regimen. Ivermectin (IVM) shows promise for early treatment.
September 2020: More than two billion doses of HCQ are distributed around the world, and the COVID-19 pandemic is contained. Early treatment with antibiotics such as doxycycline, azithromycin and IVM is endorsed by the CDC. As schools reopen, HCQ PrEP for children is instituted in high-risk areas. Variant strains of SARS-CoV-2 appear, but HCQ PrEP continues to prevent serious illness. President Trump, who has taken weekly HCQ PrEP since March, tests positive for COVID-19, says it was like “a mild cold”.
November 2020: President Trump wins re-election in a landslide over Joe Biden. COVID-19 hospitalizations drop to near zero worldwide. An experimental vaccine trial fails to meet its recruitment quota. The CCP apologizes for its role in the pandemic.
WHAT IS TO COME(9-2-21):
I am expecting a brutal fall with COVID for the following reasons.
1) The vaccinated are found now to carry an extremely high viral load with viral loads 251x the level of the unvaccinated turning the vaccinated into super-spreaders.
See this Oxford Univ. paper published in The Lancet.
The link is in this article: https://childrenshealthdefense.org/defender/vaccinated-healthcare-workers-threat-unvaccinated-patients-co-workers/
2) Take the time to listen in detail to Dr. Robert Malone - MASS vaccinating during a pandemic leads to viral variants that go around the vaccine disabling any benefit from the vaccine. If you want to have benefit (especially from a risky experimental vaccine) you should only vaccinate a targeted group of recipients who are at high risk. Listen in details to his words - they are carefully chosen: "You can't vaccinate yourself out of an ongoing pandemic... it's fundamental virology... It will drive vaccine resistant mutants." https://www.youtube.com/watch?v=4jAZuNwopIM
3) The general survival rate for COVID is high (more on that below). However it has been found that those who receive the vaccine have highly reduced immune system function to protect against pathogens. Your body produces T-cells that help to identify and attack cells that have been infected by foreign organisms (eg. cancer and other diseases). The T-cells also stimulate other cells to produce 'neutralizing antibodies' that attack infections.
However, this finding is that the vaccines suppress T-cells levels in the vaccinated... “So, the key message from our finding is we found that recipients of the Pfizer vaccine, those who have had two doses, have about five- to six-fold lower amounts of neutralizing antibodies,” David Bauer, head of the Bauer Lab in the Francis Crick Institute.
“Now, these are the, sort of, gold standard, private security antibodies of your immune system which block the virus from getting into your cells in the first place. So, we’ve found that that is less for people with two doses. We also found that for people with only one dose of the Pfizer jab that they are less likely to have high levels of these antibodies in their blood.”
Clip: https://www.youtube.com/watch?v=cb2clpCk5gw
4) The first attempt at a COVID mRNA vaccine was in 2012 for treatment of the SARS COVID virus. The vaccine was successful in driving-up the levels of COVID antibodies but it was found that in animal tests that the test animals died when re-exposed to COVID due to hypersensitivity to COVID that developed. The SARS vaccine program was cancelled We'll see how this goes for COVID-19. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3335060/
5) To date, 94% of the deaths have been in people with pre-existing health conditions and the majority have been over 70 years old. Overall, the survival rate is 99.8% (see below) for everyone however the survival rate for those under 60 yrs is extremely high. Dr. Peter McCullough notes that the early treatment protocols using standard drugs in the first few days of infection lead to 85% reduction in hospitalizations and deaths.
With weakened immune systems, new variants driven by mass vaccination, and potential hypersensitivity of the vaccinated to future exposure to COVID, it is not a great outlook.
Survival Rates prior to mass vaccination programs
Age Infection Survival Rate
0-19 99.9973%
20-29 99.986%
30-39 99.969%
40-49 99.918%
50-59 99.73%
60-69 99.41%
70+ 97.6% (non-institutionalized)
70+ 94.5% (all)
Source: https://www.medrxiv.org/content/10.1101/2021.07.08.21260210v1
Stay healthy with exercise and keep taking high-dose Vit-C, Vit-D, and Zinc
If you or anyone you know gets sick, here are the standard drug treatment protocols that have been used with such great success when used early:
Front Line COVID-19 Critical Care Alliance
Prevention & Treatment Protocols for COVID-19
https://covid19criticalcare.com/covid-19-protocols/
These vaccines hit the market with an Emergency Use Authorization allowing sale with only 6 months of safety testing vs. the normal 4yrs to 6yrs of testing for a new vaccine.
Nobody should be surprised.
6) THE SOLUTION:
Civil Disobedience, VOTE THEM ALL OUT, Bureaucracy must go
All office holders are responsible- no matter what party
(this is our best chance to vote in candidates that will truly downsize government)
APPLY THE NUREMBERG CODE TO ALL RESPONSIBLE PARTIES
Gaining Traction:
